Are you a team member in a veterinary practice?
Are you a pet parent planning a trip with your furry pal?
Veterinary Record Keeping Requirements: A Complete Guide
A lot of veterinary teams meet the same moment sooner or later. A client calls in a rush because their pet is flying soon, a certificate needs to be finalized, and suddenly someone is digging through notes from exam rooms, vaccine logs, lab results, and old email threads trying to rebuild a clean medical history.
That scramble is usually not caused by bad medicine. It's caused by inconsistent documentation.
Veterinary record keeping requirements can sound dry, but in practice they shape everything from patient safety to client trust to whether your front desk spends ten calm minutes on a request or loses an entire afternoon chasing missing details. Good records make hard days easier. Weak records turn routine work into a hairball.
Why Good Record Keeping Is a Vet's Best Friend
The most painful record problems rarely show up during a normal appointment. They show up when the pressure is on.
A patient comes in for follow-up care with a different doctor. A client disputes what was discussed at discharge. A boarding facility wants proof of vaccination. A pet owner needs travel paperwork fast and the clinic has to confirm dates, product details, and prior recommendations. If the chart is complete, the team moves. If it isn't, everyone starts guessing.
Good records protect care quality
A strong record does more than prove that something happened. It helps the next clinician know what happened, why it happened, and what still needs attention. That matters when the original doctor is off, when a specialist asks for history, or when the pet's condition changes quickly.
Good notes save future you from detective work.
That's why the best teams don't treat charting as cleanup work after the actual job. The record is part of the care itself. If a medication dose, route, or response isn't documented clearly, continuity suffers. If discharge instructions aren't captured, follow-through gets messy.
Good records also make operations sane
Practice managers see the operational side of this every day. Clear records reduce back-and-forth between CSR staff, techs, and doctors. They make callbacks faster. They make refill questions easier. They shorten the time it takes to respond to requests from clients, referral partners, and regulators.
For clinics trying to build steadier systems around compliance and documentation, this overview of practice compliance solutions for veterinary teams is a useful place to start.
The hidden value is peace of mind
There's also a less obvious benefit. Teams with reliable records are less stressed. They don't have to rely on memory. They don't have to decode rushed handwriting or wonder whether a missing detail is sitting in someone's inbox.
That peace of mind is worth a lot. In a busy hospital, the best record system is often the one that prevents panic before anyone realizes panic was coming.
The Anatomy of a Purrfect Patient Record
A compliant chart isn't just “some notes in the file.” It needs enough detail that another veterinarian can continue care by reading the record alone.
According to the Virginia administrative standard for veterinary records, compliant veterinary records require contemporaneous, legible documentation capturing ten critical data elements: client identification, patient species/breed/age/sex/weight, presenting complaint, physical exam findings, diagnostic results, procedures/treatments administered, drug dosages/routes (including lot numbers for vaccines), radiograph labels, discharge instructions, and treating veterinarian identity.

What belongs in every chart
Must-have baseline: client ID, patient details, complaint, exam findings, diagnostics, treatment details, medication specifics, discharge instructions, and the treating veterinarian's identity.
That sounds straightforward, but many records fall short in the same places. Usually it's not the diagnosis. It's the supporting details around it.
Client and patient identifiers
Start with the basics. Record the client's name and contact information, then the patient's species, breed, age, sex, weight, and any unique identifier your practice uses.Reason for visit
The presenting complaint should be easy to spot. “Limping for two days” is more useful than “not doing well.”Physical exam and findings
Document what was observed, not just the final impression. A brief but clear exam note is better than a vague summary.Diagnostics and interpretation
If tests were run, note the results and how they informed the plan. That includes imaging and properly labeled radiographs where required.
Medication details are where many charts wobble
Medication logs need to be specific. Dose, route, frequency, and duration matter. Vaccine entries should also include lot numbers where applicable. Those details aren't busywork. They support patient safety, continuity, and product traceability.
If your vaccine documentation process needs a tune-up, this practical guide to a cat vaccination record workflow is a useful model for tightening templates and staff habits.
Build templates that match real workflow
A good template doesn't create more clicking. It reduces omissions.
I usually recommend auditing your SOAP templates against front-desk intake, technician notes, doctor notes, discharge forms, and payment records. Billing information and client communication often live outside the medical note, but they still need a dependable home in the overall record system.
A lot of practices borrow ideas from broader service businesses when designing follow-up systems, reminders, and communication logs. This guide to CRM for appointment businesses gives a helpful overview of how structured client communication can support repeatable workflows.
A quick self-audit
Ask these questions:
Can another doctor take over care from this chart alone?
Can your team confirm what medication was given without asking three people?
Can you prove what the client was told at discharge?
Can you find vaccine details fast if travel or boarding paperwork comes up?
If the answer is “not always,” the fix usually starts with templates, training, and chart review habits. Not heroics.
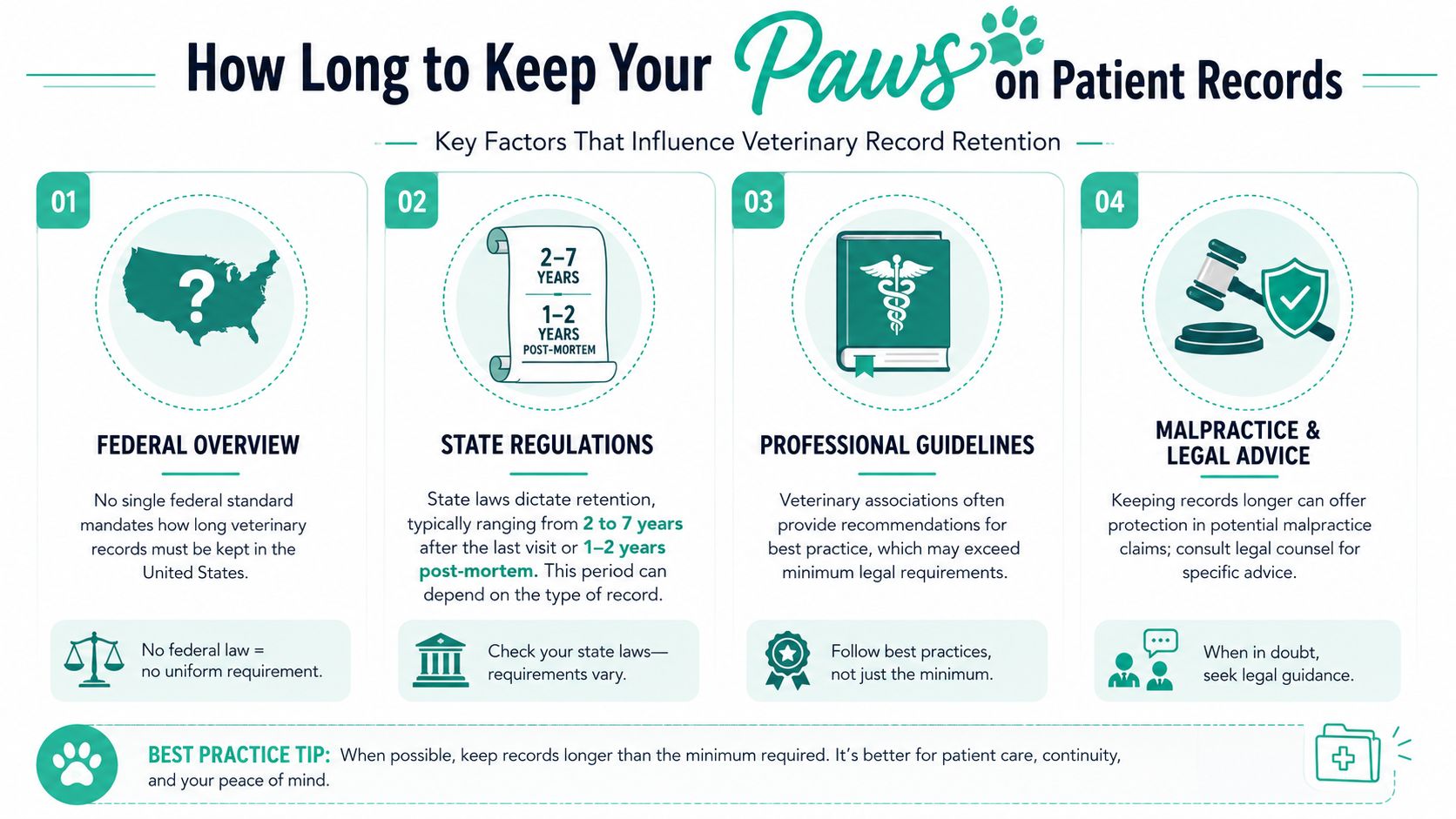
How Long to Keep Your Paws on Patient Records
Retention rules confuse a lot of clinics because there isn't one national answer in the United States.
The key point is simple: there is no unified federal standard. State law drives the retention window, and those windows vary. As summarized in this review of veterinary medical records laws by state, California requires 3 years from the last visit, Texas requires 5 years, and New York and Florida require 3 years. Because of that patchwork, many practices use the AVMA recommendation of at least 5 years as the safer working standard.
Why the simplest policy is often the best one
When rules vary by state, the cleanest internal policy is usually the one that avoids exceptions. A uniform 5-year retention policy is easier to train, easier to audit, and less likely to break when your team handles records across multiple doctors, locations, or client moves.
That doesn't turn legal complexity into legal advice. It turns a messy operational question into a manageable clinic policy.
Practical rule: If your state requires less, a five-year internal standard is often easier to run than a shorter policy with lots of caveats.
What should be retained
Retention isn't just about the final exam note. It should cover the broader treatment record, including clinical encounters, test results, medication details, and follow-up communication that supports the medical story.
For food-producing animals, the record burden is stricter. Records of veterinary medicine purchases and administration, including batch numbers and withdrawal periods, must be kept for a minimum of five years. That level of detail supports traceability and food safety.
A simple policy framework
A practical retention approach usually includes:
Area | What works |
|---|---|
Written policy | One clinic-wide retention rule, written in plain language |
Chart closure | Define when the retention clock starts, such as after the last patient visit |
Archive process | Move inactive records into a searchable archive instead of leaving them in limbo |
Destruction controls | Don't destroy anything without a documented schedule and approval path |
The biggest mistake here is inconsistency. One doctor keeps everything forever. Another purges older files. A third stores PDFs on a desktop folder nobody backs up. That's not a policy. That's a future headache with whiskers.
Paper Trails vs Digital Tails Choosing Your System
Paper charts can still work. Digital systems can also fail badly. Format alone doesn't solve compliance.
The question is whether your system helps the team create complete, timely, readable records without extra friction. That matters because the AAVSB Model Regulations for Medical Recordkeeping say records must be completed no more than 48 hours after the clinical encounter.
Where paper still helps
Paper is familiar. It doesn't crash. Some clinicians still think faster with a pen in hand, especially during high-volume treatment blocks or farm calls.
But paper has stubborn limits:
Legibility problems can turn a simple review into a guessing game.
Single-location access means one chart can't be in two hands at once.
Storage and retrieval become slower as your archive grows.
Where digital usually wins
Digital systems tend to do better when a practice wants consistency. Templates can prompt required fields. Search functions help staff pull records quickly. Permissions can limit access by role. Backups reduce the risk of one spilled coffee ending a chart's life.
That said, digital systems only help if the clinic uses them well. Bad templates create copy-paste junk. Weak permissions expose too many people to records they don't need. No backup plan means your “organized” system is one outage away from chaos.
A side-by-side practical view
System | Strength | Common weakness |
|---|---|---|
Paper | Fast for freehand notes | Hard to search and share |
Digital | Easier standardization and access | Easy to over-template and under-think |
One issue that comes up often in digital workflows is signatures. If your practice uses consent forms, treatment approvals, or digital acknowledgments, staff should understand the basics of what makes them acceptable. This overview from PDFWix on electronic signature legality is a helpful plain-English reference.
If you're cleaning up files, naming conventions, or access rules, these document management best practices for veterinary teams can help tighten the system.
The best setup is the one your team can follow every day. Fancy software won't save a clinic that charts late and inconsistently. A modest system with good habits often performs better.
Common Pitfalls and How to Fetch Your Way Out
Most record problems aren't dramatic. They're small misses that stack up.
A missing weight. An unlabeled vaccine entry. A discharge note that never made it into the chart. A callback discussed by phone but not documented. None of these feels catastrophic in the moment. Together, they create a record that can't carry the clinical or administrative load placed on it.

The mistakes that show up most often
Here are the patterns I see repeatedly in practice operations:
Incomplete medication entries
The chart says a drug was given, but not how much, by what route, or for how long.Late notes
The care happened. The charting lagged. Then details got fuzzy.Unclear abbreviations
Internal shorthand saves seconds for one person and costs minutes for everyone else.Split documentation
Part of the story is in the PIMS, part in email, part on paper, and part in someone's memory.
Fix the process, not just the chart
The strongest correction is usually structural. Don't tell staff to “be more careful” and hope for the best. Change the workflow so the right thing is easier.
Try this:
Lock in required fields for medication, diagnostics, and discharge steps.
Use end-of-visit chart checks before the patient leaves.
Standardize abbreviations or eliminate the ones that cause confusion.
Train CSRs and techs on what belongs in the record, not just doctors.
A chart should answer routine follow-up questions without requiring a scavenger hunt.
The unpaid invoice trap
One of the trickiest issues is record release when a client still owes money. Teams get frustrated, and understandably so. But frustration isn't a policy.
The Massachusetts Veterinary Medical Association FAQ highlights a key blind spot around withholding records when a client has an outstanding balance. In pet travel situations, international rules don't recognize fee disputes as valid grounds for withholding time-sensitive health documentation. That means a local billing dispute can turn into a travel failure very quickly.
Practices get into trouble by thinking only about accounts receivable and not about the downstream consequence. If a pet owner misses a travel deadline because records were held back, the clinic may end up dealing with a much bigger conflict than the original invoice.
A safer approach
A practical, lower-risk approach is to separate billing collection from record release procedures. Handle unpaid balances through your standard financial process. Handle medical record requests through a written release policy that staff can follow without improvising.
That won't solve every hard conversation. It will stop avoidable ones. And that's a pretty good trick for any clinic trying to stay out of the doghouse.
Preparing for Audits and International Travel
The clinics that handle audits calmly usually aren't doing anything flashy. They've built records that are easy to retrieve, easy to review, and easy to explain.
Audit readiness starts long before anyone asks for documents. It lives in naming conventions, completion habits, vaccine logs, signatures, communication records, and where your team stores supporting files.
What audit-ready looks like day to day
A practice is in decent shape when it can quickly produce a chart that tells a clean story from intake to follow-up.
That usually means:
Records are legible and organized
Supporting documents are attached to the patient file
Medication and vaccine details are easy to verify
Staff know who can release records and how
When an audit request comes in, the goal isn't brilliance. The goal is retrieval without panic.
Travel cases raise the standard
International pet travel adds a layer many general workflows aren't built for. A standard patient chart may support care perfectly well, but travel paperwork often depends on exact vaccine details, timelines, product information, exam dates, owner information, and country-specific documentation standards.
That's why ordinary record keeping and travel preparation need to connect. If the core chart is weak, the travel packet usually becomes a rushed cleanup project.
Here's a look at a platform used in that workflow:
For clinics handling pet travel regularly, staff also need to understand the credentialing side. This guide to USDA veterinary accreditation and travel documentation is a helpful operational reference.
Turn record quality into a service strength
Practices sometimes treat travel certificates as an annoying extra. That's understandable, but it misses the bigger point. Strong records make these cases manageable. Weak records make them disruptive.
When a clinic can produce complete history, vaccine proof, and exam documentation quickly, it becomes easier to offer pet travel support with confidence. That's good for clients, better for staff sanity, and often a sign that the underlying medical record system is healthy too.
Frequently Asked Questions on Vet Records
Can a clinic charge for copies of records
That depends on state rules and clinic policy. The safest operational move is to use a written release process and make sure staff know when records must be provided, how requests are documented, and who approves the release. If your clinic charges administrative fees where allowed, keep that separate from urgent care or travel-sensitive decision-making.
What's different about records for food-producing animals
The standard is stricter. For food-producing animals, records of veterinary medicine purchases and administration details, including batch numbers and withdrawal periods, must be retained for a minimum of five years. Those records support traceability and food safety, so they need to be complete and easy to retrieve.
Are electronic signatures acceptable
They can be, but the important issue is whether your process creates a reliable record of consent or acknowledgment and fits the rules that apply to your setting. Don't assume that a typed name in a random field is enough for every purpose. Build a consistent process and review it with appropriate advisors when needed.
How fast should records be finished
Fast enough that the chart reflects what happened while details are still fresh. If chart completion drifts, accuracy usually drifts with it.
What's the easiest improvement a busy clinic can make
Tighten the template before you buy new technology. A clean record form with required fields for medications, diagnostics, discharge instructions, and client communication solves a surprising number of daily problems.
If your practice handles pet travel cases, Passpaw helps organize the international health certificate process in a way that fits real clinic workflows. It's built to reduce document errors, keep travel requirements clear, and make life easier for both veterinary teams and pet owners.

More articles
From regulatory changes to best practices for veterinarians and pet owners, our resources keep you ahead of the curve.



